


Business Inquiry
Global:
Email:marketing@medicilon.com
+1(781)535-1428(U.S.)
0044 7790 816 954 (Europe)
China:
Email: marketing@medicilon.com.cn
Tel: +86 (21) 5859-1500



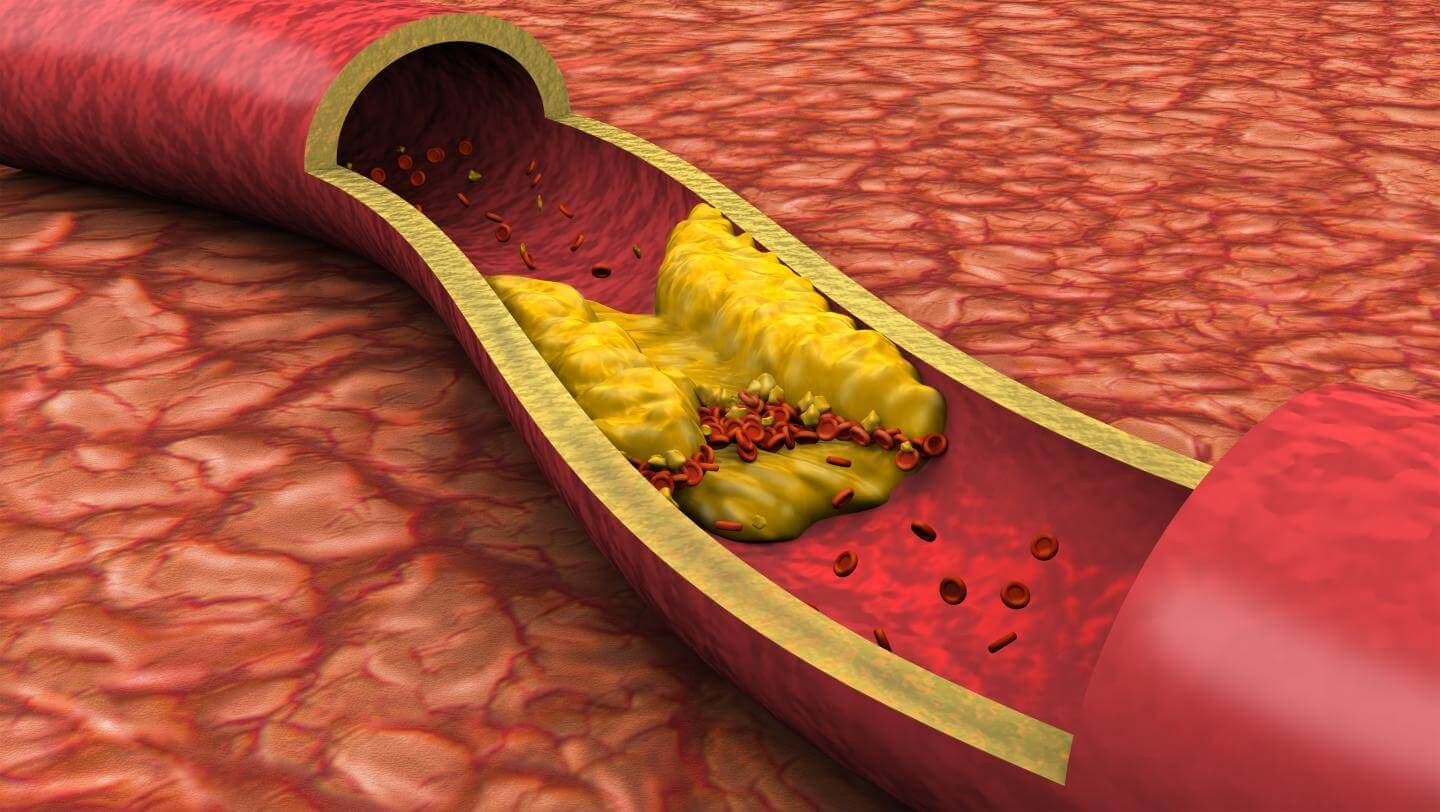
Atherosclerosis is a condition in which plaque builds up inside the arteries, leading to hardened, narrow, or even blocked arteries. The damage caused by atherosclerosis may contribute to a range of cardiovascular conditions, such as coronary heart disease or peripheral artery disease.
Scientists are rethinking their views on the relative dangers soft and hard atherosclerotic plaque deposits pose to heart health. Findings of a new study by researchers at the Intermountain Medical Center Heart Institute may be a “game-changer” for determining who’s at risk of a heart attack, they say.
The belief that soft plaque is more likely to rupture and cause heart attacks than hard calcium deposits in coronary arteries may be incorrect, according to new research that was be presented at the American College of Cardiology Scientific Sessions in Washington D.C. The find challenges views on the relative dangers soft and hard atherosclerotic plaque deposits pose to heart health.
“We previously thought the lipid-laden soft plaque was more likely to rupture and cause heart attacks, but based on our new research, it’s more the calcified plaque that appears to be associated with adverse cardiovascular events” said Brent Muhlestein, M.D., one of the study’s authors and co-director of cardiology research at the Intermountain Medical Center Heart Institute in Salt Lake City.
Intermountain Medical Center Heart Institute investigators had earlier teamed with Johns Hopkins School of Medicine and National Institutes of Health scientists to analyze the composition of plaque from 224 patients who had diabetes, but no heart symptoms. This new research reflects more long-term findings after patients were followed for an average of nearly 7 years to see if their plaque composition had predicted whether they’d have a cardiac event.

In this study, through quantitative evaluation, the composition of coronary artery plaque identified in the subjects through CT coronary angiography was stratified proportionately into amounts of soft, calcified, and fibrous plaque and compared with future risk of unstable angina, heart attack, or death. Unexpectedly, proportionately higher quantities of calcified plaque best predicted major adverse coronary events, while soft plaque did not, researchers found.
Dr. Muhlestein said further studies are needed to verify the findings, but results from his team’s research may represent a potential paradigm shift. “We need further validation to gauge the importance of why the coronary calcium score is so predictive,” he said.
Although a build-up of coronary calcium doesn’t go away, doctors can successfully treat the patient aggressively with statins. They know no one gets coronary calcium if they don’t have plaque, even if it hasn’t been seen, so anyone with coronary calcium also has atherosclerosis.
“It’s a disease marker, not a risk marker. And we think it’s possibly a very important predictor,” said Dr. Muhlestein, who noted that having a calcium score of zero is like having a 5-year warranty against heart attack, even with high levels of low-density lipoprotein, also known as LDL, or bad, cholesterol.
“The finding potentially could mean a lot of patients may not require statin therapy, even though they have high cholesterol,” he said. “Maybe we can find and identify them. If there’s no atherosclerosis, you’re not going to have a heart attack. So the coronary calcium score may allow us to much more effectively select who we treat.”
The next step for the researchers is to complete more of the scans to see if the finding holds up, which will make findings more robust.
 Relevant
news
Relevant
news







 marketing@medicilon.com
marketing@medicilon.com



